Dear friends of ICOSIM and
jawbone osteoimmunology,
It is recommended to read the current S2k guideline (long version) on radiation exposure DVT-justifying indication from both the perspective of patient protection and forensic aspects.
Here are four points from the perspective of radiation-free ultrasound sonography in dental, oral, and maxillofacial medicine for science-oriented ICOSIM members:
1.I. Dental digital volume tomography – DVT
AWMF registration number: 083-005 Status: December 2022 Valid until: December 2027
The implantological operator should be aware of the increased radiation exposure associated with DVT compared to two-dimensional imaging.
…However, three-dimensional imaging may still be justified for orofacial pathologies and diseases of the jawbone as well as a number of specific indications (European Commission 2012; Kapila and Nervina 2015; P. Jaju and S. Jaju 2015). The justifying indication requires the determination that the health benefit of the application outweighs the radiation risk. Other procedures with comparable health benefits that are associated with no or lower radiation exposure should be considered in the evaluation.
…Whereby the radiation exposure caused by an X-ray examination is to be limited as far as possible in accordance with the requirements of medical science (ALARA principle). When selecting the respective procedure, it should be taken into account that DVT application is associated with at least 10 times the effective dose compared to intraoral tube or bite-wing radiography.
Since there is still insufficient evidence for the use of DVT technology in childhood and adolescence for many questions, the indication must be carefully weighed on a case-by-case basis (European Commission 2004; European Commission 2012). A replacement production of a DVT recording exclusively for subsequent calculation of two-dimensional recordings (e.g. panoramic reconstruction or remote X-ray lateral recording) is not justified for radiation protection reasons.
In the application, the internationally established ALARA principle should generally be followed. Increasingly, the ALADA (as low as diagnostically acceptable) principle is also applied, which focuses on optimizing radiation dose in medical imaging, as proposed by the National Council on Radiation Protection and Measurements (NCRP) (White et al., 2012; Yeung, Jacobs, & Bornstein, 2019).
Risk assessments are difficult at low dose levels and are mainly based on the evaluation of cohorts of survivors of the atomic bombings in Japan in 1945 in combination with the internationally accepted “Linear No Threshold (LNT) assumption” in radiation protection (BEIR, 2006).
The estimated risk of dying from exposure to ionizing radiation from a DVT scan (risk of exposure-induced death (REID)(BEIR 2006)) is on average six cases per million (Pauwels et al., 2014), with women having a 40% higher risk than men on average (Pauwels et al., 2014). Another study calculated twice the risk for ten-year-olds compared to thirty-year-olds (Yeh & Chen, 2018).
In accordance with the optimization principle known in radiation protection, the possibilities for using dose-saving techniques, especially in the production of DVT images in children and adolescents as well as the S2k guideline “Dental digital volume tomography” long version as of December 2022© ARö, DGZMK 16 should be exhausted as far as possible (Federal Government of Germany 2018).
II. Bone density and DVT
In addition, it should be noted that structures located outside the image-generating FOV can lead to increased image noise due to the local tomography effect (Arai et al. 1999; Daatselaar, van der Stelt, and Weenen 2004; Katsumata et al. 2009).
For example, in peri-implantitis diagnosis, diagnostics of the immediate peri-implant environment (such as osseointegration of a dental implant) is only possible to a limited extent due to artifacts in DVT and CT (Draenert et al. 2007; Schulze, Berndt, and d’Hoedt 2010). To what extent DVT is possible against the background of existing imaging errors in the immediate vicinity of implant imaging cannot be reliably clarified based on current scientific data.
III. Is Hounsfield validated in DVT?
Currently, there are no randomized or controlled studies in patients that demonstrate the benefits of three-dimensional diagnostics with regard to the quality of surgical outcomes and/or the frequency of complications in implantology.
However, it should be noted that comparisons of noise between DVT devices or with CT are currently not valid, as the required calibration of Hounsfield units is not currently available on any DVT device (Blendl et al. 2012; Pauwels, Jacobs et al. 2015).
The gray values displayed in DVT are not standardized, unlike the values normalized over the Hounsfield scale in CT. Therefore, a quantitative use of gray values in DVT images, such as for bone density estimation, is not possible between different devices (Bornstein, W. Scarfe et al. 2014).
IV. Conclusion
a) Radiation exposure is harmful; its immunological safety is not proven. The Linear No Threshold (LNT) assumption applies internationally. There is no reliable “threshold” because the summation effect of radiation doses contradicts their health sustainability.
b) Image noise and imaging errors in the immediate implant environment limit DVT statements.
c) Hounsfield units in DVT are neither validated nor reliable.
d) Everyone should think further about their medical and forensic responsibility!
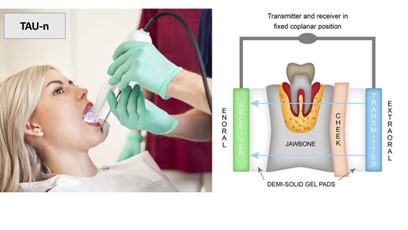
Therefore, the following principle applies, which you will also learn in training courses such as a CaviTAU® training: First OPG, then ultrasound examination, and only if the ultrasound examination is positive, then DVT due to radiation protection law (ALARA principle).











{kind=link}